A query from a parent:
“My son was just diagnosed with Pendred syndrome. He already has hearing aids from when we discovered he has hearing loss when he was 8 months old, but he needs stronger ones now because his hearing got much worse. The doctor said that he may end up deaf and that we need to check his thyroid, too. My son is already getting PT with early intervention because he is not walking yet at 18 months but we’re going to put him in speech therapy, too. What is Pendred syndrome and is it true my husband and I gave it to him? Will the therapy help with his hearing? There’s so much technical stuff and I’m really worried.”
Dear Worried Mom,
Of course you are worried. It would be overwhelming for any parent to have their child diagnosed with a problem, let alone one that can continue to affect them and that may change with time. A good step is to seek more information–as you are doing now, and hopefully will continue to do.
I’m glad that your son is already getting amplification (i.e. hearing aids) and that they are going to be adjusted/changed to reflect the change in his hearing–this is very important, and is a big step of helping him develop the best way possible. Am glad that he’s getting PT, too, if his motor skills can use some help; and that you are going to begin Speech-Language-Therapy with him, to ensure he makes the most out of his hearing and that his speech and language can develop as well as possible.
I hope that your pediatrician and the clinicians you’ll be working with (in Early Intervention, the ENT, the Audiologist, etc) will refer you to more information about Pendred syndrome, hearing loss, and rehabilitation of hearing loss in young children. Do let them know you are concerned and discuss your worries with them–I am quite confident that they will have resources, support, and more specific answers for you.
In the meanwhile, here’s a summary of some of the main features and issues in Pendred syndrome. This is not in any way a comprehensive review of Pendred or what the course of it would be in your son’s case. Nor is it a specific recommendation as to what to do in your son’s case, but I hope this overview will nonetheless give you some information to start with.
Pendred syndrome is a genetic disorder that causes early hearing loss in children. The syndrome is named after Vaughan Pendred, the physician who first described people with the disorder. It is actually the most common syndromal form of deafness in children–it is estimated that Pendred syndrome accounts for 5-10% of hereditary deafness cases! It is an autosomal recessive disorder (which basically means that both parents need to be carriers of the recessive gene–but the parents often have no symptoms and often don’t know that they carry the gene), and is associated with abnormalities of the cochlea, sensory-neural hearing loss, and diffuse thyroid enlargement (goiter). It can also sometimes create problems with balance.
Children who are born with Pendred syndrome may begin to lose their hearing at birth or soon after birth (like in your son’s case), and often lose hearing by the time they are three years old. The hearing loss is sensory-neural in type. When hearing is present at birth, it will usually worsen over time, with some children with Pendred syndrome becoming totally deaf (but not all, some children do have residual hearing or a lesser hearing loss). The hearing loss in Pendred syndrome is usually bilateral (in both ears), although one ear may have more hearing loss than the other.
Childhood hearing loss has many causes. Researchers believe that 50 to 60 percent of cases are due to genetic causes, and 40 to 50 percent of cases are from environmental causes (e.g. substances that damage the inner ear, such as certain antibiotics or chemotherapy medications).
The first part of a diagnosis of Pendred syndrome often includes the discovery of a hearing loss via a child failing a screening test or the presence of a hearing loss being found. Not all hearing loss in childhood is related to Pendred Syndrome, so the clinicians evaluate many things before considering the diagnosis and it can indeed take a bit of time before things are known for sure. Things like the kind, timing, amount, and pattern of hearing loss; the anatomy of the inner ear structures; the child’s balance and thyroid, etc. All these can help the health care professional determine whether to seek genetic testing and imaging tests for the inner ear, and to conclude whether a child has Pendred syndrome or some other type of progressive deafness.
Pendred syndrome can make the thyroid gland grow larger (when a thyroid gland grows too large and can visually bulge on the lower neck, it is called a goiter). The thyroid is a small, butterfly-shaped gland in the front of the neck, just under the ‘Adam’s apple’ and just above the collarbones. It plays an important role in the way the body uses energy from food, as well as in normal growth and development. Some thyroid issues in childhood (e.g. Grave’s Disease) can cause growth problems. However, in Pendred syndrome children often develop properly even if their thyroid is affected and their levels of thyroid hormones are usually normal. Not everyone with Pendred syndrome gets a goiter, and it typically develops in adolescence or early adulthood. Not all goiters are problematic, but if a goiter becomes large, it can impact breathing and swallowing and then treatment may be necessary. So an endocrinologist (doctor trained with diseases and disorders that involve the hormonal/endocrine system) is probably a good person to get involved even if only for followup.
By the way, it is still not clear to scientists why some people with Pendred have more issues than others (e.g. some have goiter and others don’t).
Alongside hearing loss, Pendred syndrome also can affect the vestibular system, which is the system which controls balance. The good news is that most children and adults with Pendred learn to adapt to whatever vestibular dysfunction they have and can manage routine tasks and daily balance requirements well. That said, because of the vestibular issues, some babies with Pendred syndrome may start walking later than other babies.
To get a bit technical: It is believed that Pendred syndrome is caused by mutations (i.e. changes) in a gene called SLC26A4(formerly known as the PDS gene) on chromosome 7. To be born with Pendred syndrome, a child would need to inherit two mutated SLC26A4 genes—one from each parent. Because it is a recessive gene, the parents are only carriers of the mutation (i.e. they don’t have the syndrome themselves). In a family where both parents are carriers, a child has a chance of 1:4 to be born with Pendred, and a 1:2 chance to be born a carrier. It is often recommended that if people are concerned about the possibility of Pendred (e.g. in a child or future children) that they seek genetic testing and counseling.
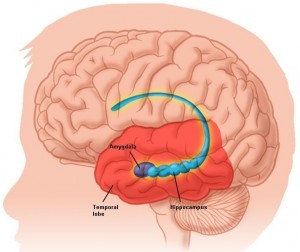
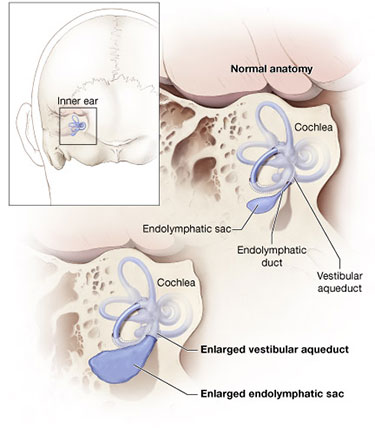
The anatomy of the inner ear is often viewed through imaging techniques such as magnetic resonance imaging (MRI) or computed tomography (CT), which allows viewing the cochlea and the vestibular system. The cochlea is the spiral-shaped part of the inner ear that converts sound into electrical signals that are then sent along to the brain through the auditory nerve. A healthy cochlea has two-and-a-half turns, but some persons with Pendred syndrome may have a cochlea with only one-and-a-half turns. The vestibular system includes a part called vestibular aqueduct. It is a kind of a bony canal that runs from the vestibule (the part of the inner ear between the cochlea and the semicircular canals) and the inside of the skull. Inside the vestibular aqueduct there is a fluid-filled tube called the endolymphatic duct, which ends with a balloon-shaped sac. People with Pendred syndrome may have an enlarged vestibular aqueduct, and the endolympatic duct and sack may also be enlarged.
Below is an image of the inner ear in some people with Pendred syndrome, taken from: http://www.nidcd.nih.gov/health/hearing/pages/pendred.aspx

When it comes to helping children with Pendred: First of all, to minimize the risk of worsening hearing loss, children with Pendred syndrome may be advised to wear head protection when engaged in activities such as bicycle riding and skiing (to avoid trauma to their head). They may be advised to avoid contact sports or situations that can lead to extreme, rapid changes in pressure such as scuba diving or hyperbaric oxygen treatment.
Like with your son, the treatment of children with Pendred syndrome indeed often involves a team of specialists. These could include an audiologist, speech-language-pathologist, otolaryngologist, endocrinologist, geneticist, physical therapist, and primary care physician. Not all need to see the child all the time, and not necessarily throughout childhood, but it is always good to have those who are working with the child communicate with each other as need be so that they can coordinate goals and needs and work as a team. Don’t be shy about asking professionals to collaborate–they can’t and won’t do so without your consent.
Hearing amplification (hearing aids, and for those who need them: cochlear implants) can greatly minimize the impact of hearing loss on language and development. Children with Pendred syndrome should start early treatment with a speech-language-pathologist, to help gain communication skills and learn how to maximize their use of their hearing aids or cochlear implant. So I think it is probably an excellent thing for your son to begin with an SLP now, when any gaps or difficulties, if there are any, hadn’t had a chance to grow wide. In addition to hearing rehabilitation through working on discriminating, identifying, understanding, and processing sounds and language better, speech-language-pathologists can also help children with Pendred syndrome with speech, voice, and language development. The hearing itself may not be made better, but how the child used the hearing they have can be get a lot better with treatment. Treatment can help minimize the impacts of hearing loss on development, language, communication, and learning. Physical therapy can help with balance issues, and help aid with motor-goals (such as walking, and later running, climbing, and so on).
It seems that your son is already up to a good start, by having a parent who is interested in getting more informed about his condition and who is seeking to follow through on the best treatment plan for him. I wish you and your son all the best, and a lovely, joyful, satisfying healthy childhood.






















You must be logged in to post a comment.